Introduction
Recognition of mental health problems within the medical profession has led to various efforts to study this problem and the risk factors involved in their presentation, such as long workdays at the hospital, work overload, sleep deprivation, complaints from relatives and patients, insufficient medical knowledge, informal learning, uninspiring academic environments, a high degree of competitiveness, and changes in their work and personal environment, which sometimes involves moving away from their families or places of origin (Prieto-Miranda, Rodríguez-Gallardo, Jiménez-Bernardino, & Guerrero-Quintero, 2013). It has been observed that from the early stages of medical training, the presence of depression or depressive symptoms is reported in 10% to 25% of students (Schwenk, Davis, & Wimsatt, 2010), while nearly half of them experience burnout and 10% suicidal ideation (Dyrbye et al., 2008), with suicide being the second cause of death in this population (Whitcomb, 2004; Anderson, 2018). At the same time, physicians in training experience various barriers in help seeking such as long waiting times to receive care, concern that their medical records will affect their ability to secure employment or work licenses in the future, stigma, and lack of time (Karp & Levine, 2018).
The nature of medical education would seem to contribute to this disparity, since on admission, medical students score better on mental health indicators than students of a similar age (Brazeau et al., 2014), yet as the medical training process advances, there is an increase in depressive symptoms (Mata et al., 2015), burnout (Dewa, Loong, Bonato, Trojanowski, & Rea, 2017), substance use (Martínez-Lanz, Medina-Mora, & Rivera, 2005) and suicide risk, the latter being the leading cause of death in men engaged in a medical residency program, and the second leading cause in women (Yaghmour et al., 2017). Specialty studies in medical residencies correspond to a period in which an increased risk of presenting with mental health problems has been observed, which has been related to long workdays and a heavy workload, increased patient care responsibilities, sleep deprivation, and workplace bullying (Levy, 2018).
In Mexico, although studies have been carried out to undertake a mental health diagnosis of resident physicians, very few include different institutions (Prieto-Miranda et al., 2013). Jiménez-López, Arenas-Osuna, and Angeles-Garay (2015) conducted a prospective, longitudinal study of 108 resident physicians at the Specialty Hospital, Centro Médico Nacional La Raza of the Instituto Mexicano del Seguro Social, in which a six-month follow-up found an increase in the prevalence of depression from 3.7% to 22.2%, anxiety from 38% to 56.5%, and suicide risk from 1.9% to 7.4%. It is a well-known fact that medical residents have a high risk of developing burnout syndrome, characterized by depersonalization, emotional fatigue, and a decrease in the effectiveness of their work, which is linked to depression, affecting the personal and family structure, and reflected in job quality and performance (Pérez Cruz, 2006), as well as a deterioration in their quality of life (Prieto-Miranda et al., 2013).
This study seeks to determine the mental health conditions and associated factors in medical residents in the Guadalajara Metropolitan Area, which can serve as the basis for proposals to improve the well-being, quality of life, prevention, and care of specialists in training.
Method
Study design and subjects
This is a descriptive, cross-sectional, and observational study, whose inclusion criteria were all phisicians undergoing a regular process of specialized training at one of the hospitals (Secretaría de Salud, IMSS or ISSSTE) available in the Guadalajara Metropolitan Area (GMA), excluding those who were not undergoing a regular training process, had incompletely answered the survey, or had failed to sign the informed consent form. To have quick, efficient access to the sample universe, the Google Forms® tool (Rayhan et al., 2013) was used to prepare an online survey that could be answered anonymously by anyone with Internet, a computer or mobile device, and the access link, once they had signed the informed consent form.
The sample size was calculated using the formula for conducting surveys:
Where: N = Total population (2724), z = 1.96 squared (95% certainty), p = expected proportion of response (in this case 50% = .5) and e = margin of error (5%), yielding n = 337.
The invitation to participate was voluntary and sent via the WhatsApp® application using the snowball method, containing a brief description of the study objectives and inclusion/exclusion criteria, accompanied by the access link, which could be answered within a period of six months (05/01/2019 - 10/31/19), with an expected time of completion of 15 minutes.
Procedures, measurements, and categorizations
The survey was designed to yield results in three sections: 1. Sociodemographic data, 2. Self-applied clinometric tests: Goldberg’s General Health Questionnaire (GHQ-28), WHO ASSIST V-3 test, and Maslach’s Burnout Inventory (IBM), and 3. Specific job characteristics of subjects and associated risk factors.
To assess self-perceived health status, it was decided to include the GHQ28 questionnaire, widely used in epidemiological and population studies for the evaluation of mental health from the perspective of primary or preventive medicine. This self-administered questionnaire consists of 28 items grouped into four subscales (A: Somatic symptoms, B: Anxiety and insomnia, C: Social dysfunction, D: Depression) with seven items each (Lobo, Pérez-Echeverría, & Artal, 1986; García Viniegras, 1999). Two different models were used for the analysis. The first was based on the 0, 0, 1, 1 response method for the total items, which identifies probable non-cases/case (NC/C), with a cut-off point of 6/7 respectively. Using the same response method, the second analysis was performed on the subscales, with a cut-off point of 5/6 to recognize NC/C in each one.
For the early identification of health risks and disorders due to substance use, the WHO ASSIST V-3 test was administered, consisting of eight items on recent (past three months) and lifetime use of 10 different substances (tobacco, alcohol, cannabis, cocaine, amphetamines, or other stimulants, anxiolytics, hallucinogens, inhalants, and other drugs). The score obtained makes it possible to classify individuals according to the risk level for each substance: low, moderate, or high (World Health Organization [WHO], 2011).
The Maslach Burnout Inventory-Student Survey (MBI-SS) was used to measure the presence of work stress or burnout syndrome at work in its 22-item Spanish version, which assesses the three central variables characterizing burnout in health professionals: exhaustion, depersonalization, and low professional efficacy (Hederich-Martínez & Caballero Domínguez, 2016).
Eighty hours of work per week was used as the cut-off point for creating two groups for a comparative analysis, because two on-call shifts a week plus a nine-hour work schedule from Monday to Friday amount to 69 hours, while three on-call shifts per week added to the same work schedule from Monday to Friday total 81 hours.
Statistical analysis
The sociodemographic results and the results of the nominal and ordinal variables were presented through frequencies and percentages. The results of continuous variables are shown as a mean and standard deviation, while Odds Ratios (OR) with a 95% confidence interval were obtained for risk estimation. The Student’s t-test was performed for the differences in means, Pearson’s test was used to identify correlation levels between two continuous variables with parametric distribution and if they did not exist, Spearman’s test was performed. Statistically significant differences were considered when the p value was less than .05. The Levene test was performed to evaluate the equality of the variances for one variable (homoscedasticity).
At the end of the survey, results were automatically entered into a spreadsheet, and at the end of the sampling, the information was exported to the SPSS version 25.
Ethical considerations
The study was approved by the research ethics committee of the Jalisco Institute of Mental Health (Instituto Jalisciense de Salud Mental) (Verdict: 2019-197).
Results
Sociodemographic
The initial sample obtained comprised 312 resident physicians from the GMA. Six surveys were excluded from the final analysis due to errors in their completion or incomplete data, leaving a total of 306 residents included as a final sample, equivalent to 11.23% of the total residents in the GMA (n = 2724).
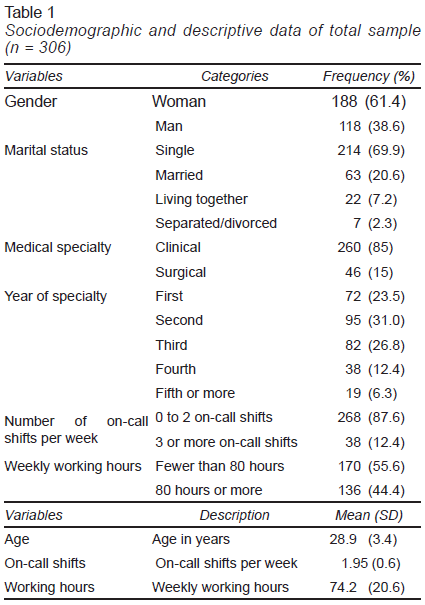
A total of 61.4% of the respondents were women and 38.6% men. Among them, 23.2% were in the first year of the specialty, 30.7% in the second, 26.8% in the third, 12.4% in the fourth, and 6.9% in the fifth year or another higher grade. 84.9% of subjects were engaged in a clinical specialty, and 15.1% a surgical one. The total mean age was 28.9 ± 3.4 years, with a statistically significant difference (p ˂ .05) from the mean of 29.1 ± 3.5 years in residents in clinical specialties, and 28.0 ± 1.9 years in surgical ones. The complete sociodemographic results are shown in Table 1.
Clinometric tests
GHQ 28
According to the total score of the scale, 58.2% of respondents had symptoms suggesting that their mental health had been affected; 23.2% showed symptoms compatible with anxiety and insomnia; 18% displayed somatic symptoms; 14.7% experienced dysfunction in the social sphere, while 9.2% had depression symptoms. Fourteen per cent of residents reported noticing that they had repeatedly thought of taking their own lives in recent weeks.
There were no differences regarding gender, specialty (surgical or medical), or on-call shifts per week. As for the NC/C frequency ratio, statistically significant differences (p < .05) were observed between those who worked over 80 hours per week (HWW) and those who worked fewer than 80 (80/90 vs. 48/88 respectively).
After the subscales had been analyzed, no differences were found for the somatic symptom subscale in relation to the NC/C frequencies regarding gender or on-call shifts per week, although statistically significant differences were observed (p < .05) regarding surgical rather than medical specialties (33/13 vs. 218/42, respectively), and in those with over 80 HWW versus those with fewer than 80 (152/18 vs. 99/37, respectively).
For the social dysfunction subscale, statistically significant differences (p < .05) were observed in the NC/C frequencies in those with over 80 HWW compared with those with fewer than 80 (152/18 vs. 109/27, respectively). No differences were found in relation to gender, type of specialty performed (medical or surgical) or on-call shifts per week variables.
There were no differences in the ratio of NC/C frequencies for the anxiety and insomnia subscale, or in depression, with respect to gender, the type of specialty they were studying (medical or surgical), on-call shifts per week or hours of work per week.
ASSIST
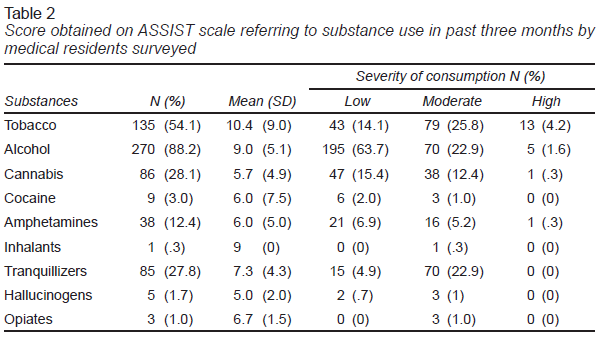
All the substances included in the ASSIST questionnaire had been used by at least one resident physician in the last three months. The three substances with the highest frequency of consumption were ethanol (88.2%), tobacco (54.1%), and cannabis (28.1%). The remaining scores obtained, and the severity of consumption are fully described in Table 2.
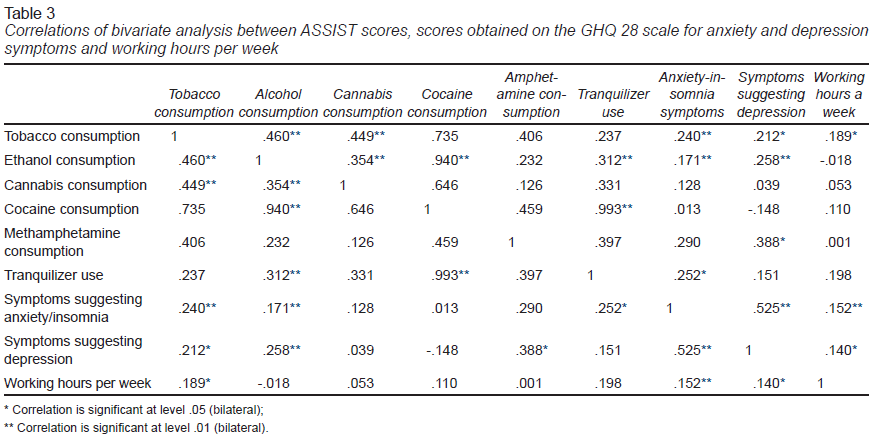
Statistically significant differences (p < .05) were observed in the ethanol consumption score in the comparison between men and women (10.2 ± 6.0 vs. 8.2 ± 4.3, respectively), and in those with over 80 and fewer than 80 HWW in the scores obtained in the consumption of tobacco (12.5 ± 10.2 vs. 8.8 ± 7.7, respectively), and tranquilizers (8.4 ± 5.1 vs. 6.5 ± 3.3, respectively). After the correlation analysis between the ASSIST scores, the scores for anxiety and depressive symptoms in GHQ 28 and HWW had been performed, a high correlation (r = .99) was found for the consumption of cocaine and tranquilizers and for the consumption of cocaine and ethanol (r = .94), as well as a statistically significant correlation between the consumption of methamphetamine and depressive symptoms (r = .388) and the consumption of tranquilizers and anxiety symptoms (r = .252); the remaining correlations are shown in Table 3. However, when Spearman’s test was used to identify correlation levels between cocaine users (n = 9), tranquilizer users (n = 85) and, ethanol users (n = 270) no results were found to be statistically significant.
The Maslach Burnout Inventory
A total of 72.5% of respondents obtained scores that placed them in the range of being at risk of experiencing burnout. Also, 59.8% presented a high risk on the subscale of emotional exhaustion, 40.2% on the subscale of depersonalization, and 31.4% on the subscale of personal fulfillment. For the gender, type of specialty (medical or surgical) and number of on-call shifts per week variables, no differences were found in the scores of the subscales, whereas in the HWW variable, statistically significant differences (p < .05) were found in the subscale of emotional fatigue in those with over and fewer than 80 HWW (32.4 ± 14.7 vs. 27.6 ± 14.0 respectively).
Specific job characteristics and associated risk factors
Workload and mental health care
The average HWW was 74.2 ± 20.6, with a statistically significant difference (p < .001) between people studying a surgical (M = 82.6 ± 23.4) and a clinical specialty (M = 72.7 ± 19.8). Out of an average total of 1.9 ± 0.7 on-call shifts performed in a week, those who worked 0-2 on-call shifts accounted for 87.6%, while those with ≥ 3 totaled 12.4%. Subjects in the surgical specialty had 2.2 ± .7 on-call shifts per week, compared with an average of 1.9 ± .7 in the clinical specialty (p < .01).
It was observed that working fewer than 80 HWW is a protective factor for not requiring mental health care services, as opposed to working over 80 (OR = .59, CI [.4, .9], p < .05), with those who reported anxiety and insomnia symptoms being at a higher “risk” of needing to receive mental health care than those who did not (OR = 2.1, CI [1.2, 3.6], p < .01).
A total of 31.4% thought that the relationship with their institution might be affected if their colleagues or the authorities knew that they required mental health care, while 50.3% did not know whether there were facilities for receiving care from their institution. Perception of this differed by gender, with more men perceiving greater ease of access to mental health services than women (OR = 2.14, CI [1.1, 4.0], p < .05).
Risk of dropping out of the specialty and workplace bullying
A total of 21.2% of respondents frequently thought about quitting, the most representative risk factors being anxiety and insomnia (OR = 5.50, CI [3.0, 10.0], p < .0001), depression (OR = 15.9, CI [6.4, 39.8], p < .001), and burnout (OR = 33.6, IC [4.6, 246.7], p < .001).
In turn, 39.2% considered that workplace bullying existed in their residency, and this subgroup showed a greater risk of presenting anxiety and insomnia (OR = 1.95, CI [1.1, 3.4], p < .05), burnout (OR = 2.17, CI [1.3, 3.8], p < .01), ≥ 3 on-call shifts a week (OR = 2.15, CI [1.1, 4.4], p < .05), and ≥ 80 HWW (OR = 2.27, CI [1.4, 3.7], p < .001).
Discussion and conclusion
There have been numerous efforts to study the phenomenon of mental health in medical training. A meta-analysis of 54 studies, including 17,560 resident physicians, found a depression prevalence of 28.8% (Mata et al., 2015), while in its report on the lifestyle and happiness of residents, Medscape notes that 10% of the residents in the United States feel depressed daily or most days, and 33% sometimes, while 9% report having suicidal thoughts (Levy, 2018). It is worth noting the relatively low proportion of people who reported depression in the survey (9.2%), especially as compared with the high percentage who reported having had “the idea of not wanting to live or taking their own lives in the past weeks” (14%). Apparently other phenomena such as burnout, anxiety symptoms, and substance use could have contributed as intervening factors (independently of depression) to the increase in the number of people with “thoughts of death.”
Depression affects people’s working lives and decreases their work effectiveness, and since they are medical personnel in training, this is an even more delicate issue, since it is associated with a high number of accidents or iatrogenesis, and deficiencies in the quality and warmth of patient care, which in turn affects the healing process (Velásquez-Pérez, Colin-Piana, & González-González, 2013).
Since certain factors facilitate involvement in drug use, such as the presence of tension, stress and, anguish caused by the demands of the role played by the subject, those engaged in the medical profession and in training are particularly susceptible to substance use. In our study, the most frequently consumed substances were ethanol (88.2%), tobacco (54.1%), and cannabis (28.1%), followed by tranquilizers (9%) and methamphetamines (6%). These data contrast with a survey conducted on 192 residents of a general hospital in Mexico City, where less substance use was reported (65% consumed alcohol, 4.5% cannabis, and 3.4% amphetamines), except for the consumption of tobacco and tranquilizers (55% and 10.6%, respectively), which was higher (Martínez-Lanz et al., 2005).
Regarding the correlation analysis, what is observed in terms of alcohol consumption and its association with other substances and intervening factors is relevant since no other substance correlated with as many variables. It could therefore be hypothesized that alcohol is usually a gateway drug, which leads to the use of other substances (in our study, it had a statistically significant association with all substances except methamphetamines). Even more striking are the levels of correlation between cocaine and alcohol and tranquilizers use. It is known that cocaine users tend to combine this substance with alcohol and subsequently abuse benzodiazepines (tranquilizers) following intoxication with the drug in question. However, given the extremely small sample of people who use this substance (nine people reported consuming cocaine, six of whom only mildly), these results should be taken with caution, especially because, when the non-parametric Spearman’s test was performed, no statistical significance was obtained for the correlation levels.
A risk of developing burnout was observed in 72.5% of our sample, exceeding the rates reported in similar surveys conducted in several countries, where it was reported that a third to half (36-51%) of physicians experienced professional burnout, depression, or both simultaneously, and that 19%-25% of the latter reported that their problem was so serious that it made them consider dropping out of medical school (Kerry, 2019). Along these same lines, our results reflect the fact that in residents who frequently thought about quitting (21.2%), there was a greater risk of developing anxiety, insomnia, depression, and burnout symptoms. Moreover, those who reported the presence of workplace bullying (39.2%) had a higher risk of developing intense symptoms of anxiety, insomnia, and burnout, as did those with a higher number of on-call shifts, as well as over 80 HWW. These data coincide with the risk variables present in the study conducted by Kerry (2019).
Despite the scope of the problem, there is a large gap in the search for mental health care in this population, where stigma seems to be the main factor preventing them from receiving specialized treatment, since it can raise doubts about whether seeking care would affect their stay in medical school or jeopardize their academic achievements (Whitcomb, 2004). It is estimated that 64% of the physicians with burnout or depression have never received care (Kane, 2019), while 68% of the residents report stigma related to mental health care seeking (Levy, 2018). The reasons cited for refusing to seek care include the fact that they prefer to handle it independently, lack of time, fear of being reported to the medical leave department, shame of receiving a psychiatric diagnosis, and fear of this having repercussions on their work (Gold et al., 2016). In our survey, nearly a third considered it disadvantageous for their colleagues or the authorities to know about their mental health care, while half, mainly women, did not know how to access these services. Those with anxiety and insomnia had a greater need to request care, compared to those with fewer than 80 HWW, who were less likely to have requested it. At the same time, fear of professional sanctions can lead to risky coping methods, such as excessive substance use or self-medication (Schwenk et al., 2010).
The limitations of our study include the fact that it is based on self-reported data, and may contain several potential sources of bias, due to the difficulties caused by selective memory, attribution, or exaggeration, as well as the selection of residents from clinical specialties included in the study rather than surgical specialties, possibly attributable to the non-probabilistic selection of the sample.
Our study contains crucial features, such as the greater number of hours worked per week, the presence of workplace bullying in the hospital to which they are attached, and the consumption of ethanol and methamphetamine, which impact the mental health of medical residents. These findings are consistent with what has been reported in the literature and enable one to identify significant areas of intervention for the improvement of academic and work conditions, to improve training processes and reduce the risks to mental health of medical specialists in training, thereby improving the quality and safety of care for the user population.