INTRODUCTION
Social isolation is a known risk factor for diverse negative health-related and mental health-related outcomes among older adults. These outcomes include the development of depression and depressive symptoms (DS). This risk was recognized well before the COVID-19 pandemic (Cipolleta & Gris, 2021; Santini et al., 2020). Therefore, as the World Health Organization warned, mental health-related complications associated with social isolation could increase in this already vulnerable population due to the adoption of the lockdown periods to limit the spread of SARS-CoV-2 at the beginning of the pandemic (World Health Organization [WHO], 2020). In this sense, older adults are not only at higher risk for increased mortality from COVID-19, but are also vulnerable for its indirect adverse mental health effects, such as the development of DS (Fraser et al., 2020).
Consequently, during the COVID-19 pandemic, multiple projects have been conducted in order to study the impact that social isolation may have had on older adults’ mental health during diverse lockdown periods. In the pre-pandemic era, several studies have already shown an association between loneliness and social isolation and various adverse health-related outcomes among older adults including all-cause mortality, poor physical health (Noone et al., 2020), and increased risk for dementia (Cipolleta & Gris, 2021; Santini et al., 2020).
However, results coming from the early months of the pandemic and the first lockdown periods have been very heterogeneous, either because they did not observe changes in mental health during that period (Röhr, Reininghaus, & Riedel-Heller, 2020), or because they reported a worsening of DS (Robb et al., 2020). As the future of the pandemic remains uncertain, it is pertinent to continue studying the possible associations between isolation and its negative mental health-related consequences in older adults, such as the development of DS. Equally important is the need to study variables that could mitigate these consequences, such as maintaining social interactions (i.e., social connections). Social connections are the relationships that we have with the people around us and are shaped by verbal and non-verbal performances that co-construct the meaning of such interactions, either in person or remotely by using technology (Birt et al., 2020). For instance, studies conducted in high-income countries before the pandemic have reported that living with other people and maintaining remote contact through communication tools, such as telephone calls or videocalls, had a positive impact on the reduction of DS (Noone et al., 2020; Stevic, Schmuck, Matthes, & Karsay, 2021). However, little information from developing countries is available concerning the potential effect that the first lockdown period may have had on older adults’ mental health (Buenaventura, Ho, & Lapid, 2020). In Mexico, in order to limit the number of infections by SARS-CoV-2, between March 23 and May 30, 2020, strict social distancing (domiciliary lockdown), as well as the suspension of all non-essential activities were recommended by the Government (Ibarra-Nava, Cardenas-de la Garza, Ruiz-Lozano, & Salazar-Montalvo, 2020). Relying on the PAMCOVID telephone survey aimed at communitarian older adults, and administered during the first lockdown period in Mexico (Hernández-Ruiz, 2021), the objective of the present study was to determine the association between social connections – assessed by the housing situation (if they lived alone or in the company of someone else) and the use of communication tools (phone-calls or video-calls) to maintain contact with family, friends, and neighbors during the first lockdown period in Mexico City – and the presence of DS among community-dwelling older adults.
METHOD
Participants
Cross-sectional study including the 269 participants from the PAMCOVID telephone survey. Briefly, the PAMCOVID survey is the Mexican counterpart of the French PACOVID (“Personnes Agées face au COVID”) longitudinal telephone survey. These surveys were set up in the region of Bordeaux (France), and Mexico City a few days after the first global lockdown. Both were aimed at communitarian older adults and administered by trained health staff. Both surveys shared the initial main objective of addressing the issue; what are the attitudes, psychological, and social experiences of the older persons regarding the COVID-19 crisis and the lockdown measures? The complete methodology and initial results for both surveys have been described elsewhere (Hernández-Ruiz, 2021).
The collected data included information on the housing situation during the lockdown (i.e., if participants were living alone or with someone else), mental-health (three items from the CES-D questionnaire: how often have they felt “sad”, “depressed”, and “lonely” over the last week; Radloff, 1977), health status (including self-reported comorbidities), and social variables (non-professional phone or video contact over the last week).
For the present study, the included population consisted in older persons (≥ 65 years-old) from a Geriatrics outpatient clinic at a third-level university-affiliated hospital in Mexico City whose consultation was canceled during the first national mandatory lockdown. Thus, eligible participants were contacted, and asked if they wished to participate in a 30-minute phone interview. Data was collected in May-July 2020. At the beginning of the interview the objectives of the study were presented, and verbal informed consent was obtained. If the persons themselves could not respond to the questionnaire but wished to participate, a proxy was invited to answer in their place. Exclusion criteria were refusal to participate in the study, inability to answer the interview due to cognitive impairment or severe hearing problems as well as the absence of a proxy informant who could answer for them if needed.
Measurement
Depressive symptoms
DS were established by three items from the Center for Epidemiological Studies depression (CES-D) scale (how often in the past week have you felt sad / how often in the past week have you felt depressed, and how often in the past week have you felt lonely). Each item was scored on a four-point scale, and then it was dichotomized in “no” (not at all) or “yes” (rarely or less than a day, some of the time 1-2 days, occasionally 3-4 days or most of the time 5-7 days), being “yes” if in the past week they had felt these feelings at least one day. If the participants answered “yes” for at least one question, they were considered as having DS. If the participants reported DS they were oriented to receive the correspondent attention and also were referred to the hotline for older adults that was implemented by the Geriatrics clinic (Navarrete-Reyes & Avila-Funes, 2020).
Social connections
Several measures of social connections were included. Participants were asked about their housing condition during the lockdown period: if they lived alone or in the company of a partner/another member of the family. Likewise, they were asked if they have had remote contact via communication tools (phone calls or videocalls) with other persons (family members, friends and/or neighbors). Finally, participants were asked the number of phone calls or videocalls received on the seven days preceding the interview, and if that number represented a lower / same / higher quantity of calls respect to the usual (previous to the lockdown period).
Other variables
We obtained demographic data (age, sex, and level of education) from the medical records. Health conditions included self-reported diagnoses of hypertension, diabetes, or chronic lung disease.
Statistical analysis
Variables were described using arithmetic means and standard deviations (SD) or frequencies and proportions when appropriate. The following statistical procedures were used according to the characteristic of each variable: chi square test for qualitative data or Student t test for continuous data. In order to test the association between every measure of social connection and the presence of DS, univariate logistic regression models were conducted. All statistical tests were evaluated using 95% confidence intervals (CI) and p value < .05. Statistical tests were performed using the SPSS software for Windows® (SPSS Inc., Chicago, IL, version 25).
Ethical considerations
The patients/participants provided their informed consent to participate in this study. PAMCOVID ethics approval number 3361 (CONBIOÉTICA-09-CEI-011-2016027).
RESULTS
From 269 participants, the 71.7% (n = 193) of the responses were directly obtained from participants themselves and the 28.2% (n = 76) from a proxy. Mean age of participants was 83.2 (SD = 6.5; range 67-100), and 72.5% were women. The most prevalent chronic diseases were hypertension 66.5% (n = 179) and diabetes (n = 96; 35.7%; Table 1).
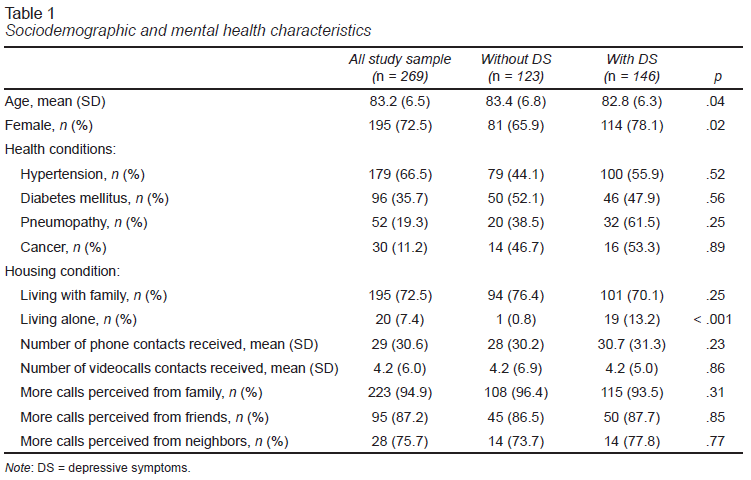
Regarding the housing situation during the lockdown period, most of the participants lived with a family member (n = 195; 72.5%). The most used means to keep social interactions were phone calls (n = 243; 90.3%) with an average of 29 (SD = 30.6) calls received from family members, friends and/or neighbors, in the seven days prior to the interview. And most of the participants perceived having received a greater number of calls (n = 231; 85.9%), being the calls from family members the ones who reported a greater perceived increased (n = 223; 94.9%), followed by the calls from friends (n = 95; 87.2%) and neighbors (n = 28; 78.5%). On the other hand, the use of videocalls was the less frequently used communication tool (n = 117; 43.5%). Among the participants that reported videocall use, an average of 4.2 (SD = 6.0) videocalls were received in the week before the interview from family members, friends and/or neighbors.
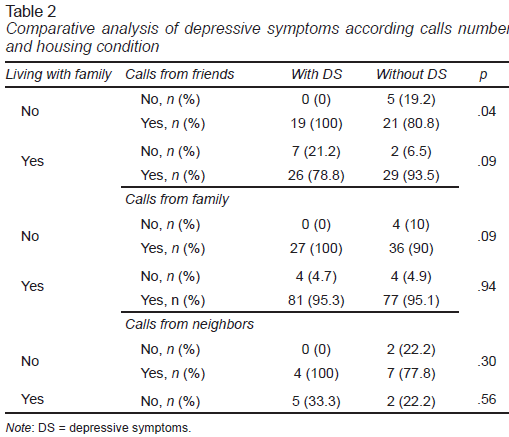
Half of the participants (n = 146; 54.3%) reported the presence of at least one depressive symptom in the week before the interview and “feeling sad” was the most frequently reported answer (n = 130; 48.3%). Compared with those who did not have DS, participants who reported DS were younger (p = .04), were predominantly women (p = .02), and more frequently reported living alone (p < .001). Despite that a higher number of received phone calls from their families, friends and/or neighbors was reported by participants with DS respect to their counterparts without DS, the difference was not statistically significant (p = .23). In the same vein, participants who had DS more frequently reported that the number of phone calls received from family, friends and/or neighbors during the lockdown was higher if compared to the pre-pandemic period; however, this difference was not statistically significant either (p = .39). In the same vein, the univariate logistic regression analysis showed that the number of phone-calls from friends (OR = .90, 95% CI = [.54, 1.4], p = .68), family members (OR = .51, 95% CI = [.26, 1.00], p = .52) and neighbors (OR = .83, 95% CI [.37, 1.8], p = .63) was not statistically significant associated with the presence of DS. However, stratifying by housing situation (living alone vs. those who lived in the company of another person), only those who were living alone and had a lower number of phone-calls from friends presented more DS (p = .04; Table 2).
DISCUSSION AND CONCLUSION
This study did not find an association between keeping social connections and the presence of DS in community-dwelling older adults. And only when stratifying by housing situation, we found that those who were living alone and had lower number of phone-calls from friends presented more DS.
During the first waves of the COVID-19 pandemic, restrictive measures such as lockdowns and physical distancing were implemented in order to protect the population, particularly the more vulnerable groups as the older adults. However, it was warned that these restrictions could become a risk factor for the development of psychological problems such as DS (Cipolleta & Gris, 2021). That is why we hypothesized that the use of communication tools, like phone calls or video-calls, and not living alone (i.e., social connections) would provide a protective effect against DS (Käll et al., 2020). Nevertheless, this study does not prove it.
Even if our results are in the same line with existing literature reporting that populations with higher risks of developing DS during the first lockdown period were younger and living alone, we failed to show a statistical and significant association between the number of calls, as a proxy for social connection, and the presence of DS. For instance, Robb and collaborators showed that in 7,127 English community-dwelling older adults, women, younger persons, those single/widowed/divorced and those who were living alone more frequently reported a worsening of DS during the first lockdown (Robb et al., 2020). However, the evidence showing that the initial lockdown did not have the impact that we might have thought is increasing. For instance, in the cohort of Röhr and collaborators consisting of 1,005 community dwelling German older adults (aged 65-94) who were being followed for depression and anxiety prior to the pandemic, the authors report that mental health-related measures remained largely unchanged during the first lockdown period. This being assessed by a computer-assisted standardized telephone interview (Röhr et al., 2020). In the same vein, van Tilburg et al. found that despite an increase in the feeling of loneliness in older people, depression and anxiety feelings remained roughly stable during the first lockdown. This was evaluated in 1,679 Dutch community-dwelling persons aged 65-102 who completed a digital survey of loneliness and mental health (van Tilburg, Steinmetz, Stolte, van der Roest, & de Vries, 2021). It is possible that this can be explained by older adults’ ability to apply coping strategies, like engaging in leisure activities, maintaining their daily routine, or by the acceptance of the lockdown situation, as a way of facing these new circumstances. Likewise, they may display lower stress reactivity and more emotional resources to adapt in better ways to face adverse situations, as suggested by the French PACOVID study (Hernández-Ruiz et al., 2021).
It is important to recall that most of the evidence recommending the use of communication tools to maintain remote social interactions is based on studies that only found a positive impact of these tools in younger populations. However, a multi-national cross-sectional online survey by Bonsaksen and collaborators conducted in community-dwelling older adults during the first months of the pandemic, reported that only the participants between 60-69 years endorsed a reduction in the feeling of loneliness and an increase in quality-of-life estimators with the use of video-based communication (Bonsaksen et al., 2021). The mean age of our sample was higher in comparison to studies that recommend the use of newer communication tools, which may influence why in our sample only 43% of participants used video-calls. Nevertheless, this proportion is larger than the reported prevalence of use in other populations, which may reflect the characteristics of the Latin-American housing, where intergenerational cohabitation is more frequent (Kinsella, Velkoff, & U.S. Census Bureau, 2002). Another factor to account is that most of the studies evaluating older adults’ mental health during the different lockdown periods have not been performed in Latin-American countries, where older adults probably experienced different impacts of the pandemic respect to their counterparts in high-income countries. Likewise, the means to keep socially active or the social connections adopted by older adults in Latin America could have been different, as suggested by the study of Tyler and collaborators. The work examined the relationships amongst demographics, COVID-19 life impacts, depression and anxiety in adults aged 60 or older from 33 countries (Tyler et al., 2021). This study found that in the first months of the pandemic being separated from, and having conflicts with loved ones predicted depression, as did residing in a country with higher income. In our study, most of the participants kept their family and friends close, and most of the participants lived in the company of someone else, who most likely acted like their social connections physically and helped them to maintain contact out of the household. This may be supported by the finding that in our study we only found DS among those participants who lived alone and did receive fewer calls from friends. Which may be a representation of other social constraints in these individuals. We hypothesize that living alone constrained them to not have much contact with their family members, and consequently their friends represented their most important social relationship outside of the household. Indeed, in Geriatrics it is well recognized that living alone and being socially isolated are two factors that can have a significant impact on older adults’ mental health (Tanskanen & Anttila, 2016).
Some of our study’s limitations are the lack of a previous mental health status assessment, its cross-sectional design, its sample size and that we didn’t include participants who did not have access to phone-calls. However, several strengths can be underlined. This study is the first-one that has sought to determine whether maintaining social connections during the first lockdown either by household status, phone or video-calls had an association with the presence of DS in a middle-income country. Moreover, by relying on the telephone to do our survey, it was possible to achieve the participation of people in more vulnerable states of health, or who do not have the electronic means to answer an online survey. Which also contributes to reduce the selection bias, as described in other publications (Bethlehem, 2010). However, we are not exempt from other selection biases.
In conclusion, the present study showed that relatively younger participants, women, and people that were living alone and receive fewer calls from friends, more frequently reported depressive symptoms during the initial COVID-19 lockdown period in Mexico City. Social connections did not had associations with the presences of DS. This may reflect the impact of in person social interactions in the people who lived in the company of someone else. The results of this study offer an insight at some of the conditions that the older adults from Mexico City experienced during the first lockdown period of the COVID-19 pandemic, and thus, may promote the creation of tools to address the situation of those individuals who may have fewer social connections.