INTRODUCTION
The anxious state is characterized by feelings of fear and worry that affect mental health and cognitive functions such as attention, memory and decision making (Bishop, 2009; Paulus & Yu, 2012), crucial to maintaining a balance between health and daily, academic, and socio-emotional skills (Simpson et al., 2010). This anxious state, common in young students (Kawakami et al., 2012), was exacerbated during the COVID-19 lockdown. Fear of the unknown and the risk of dying from infection increased anxiety levels in vulnerable young people, becoming a serious public health problem (Pérez-Cano et al., 2020; Medina-Mora, 2020).
The age of onset of the first symptoms of anxiety occurs during neurodevelopment, peaking during adolescence, a period of major age-related physical and behavioral changes. Drastic adjustments in neuronal connectivity and pruning, together with changing levels of hormones and neurotransmitters, are the basis of the functional changes associated with anxiety in late adolescence (age 24), which stabilize at the beginning of adulthood (Paus et al., 2008; Solmi et al., 2022).
Gender differences in anxiety have been described, with women having higher prevalence rates as well as more severe clinical symptoms (Asher et al., 2017). However, despite these differences in the prevalence rates of anxiety disorders, the age of onset of anxiety disorders does not differ between genders (De Lijster et al., 2017).
Anxiety is an adaptive reaction to stimuli regarded as threatening, accompanied by autonomic, neurophysiological, and psychic changes (Cattell & Scheier, 1958; Lazarus & Averill, 1972; Spielberger, 1972). According to Spielberger, in crisis situations, the immediate emotional state can be altered and modified over time depending on the biological, environmental, and social personal characteristics that explain, modulate, and maintain behavior (Spielberger, 1972).
Anxiety has various dimensions, determined by the intensity, frequency and duration of the manifestations and existence of comorbidity. It can occur as a momentary state (state-anxiety, SA) or be an intrinsic characteristic of individuals (trait-anxiety, AR). In other words, it is no longer a transitory emotional state, but a relatively stable tendency to perceive multiple situations as threatening (Spielberger, 1972; Saviola et al., 2020) and both SA and TA are evaluated using the Spielberger State-Trait Anxiety Inventory (STAI).
When these manifestations of anxiety are intense, recurrent, and also compromise social and emotional functionality and everyday activities, they are classified by the DSMV (American Psychiatric Association, 2013) as generalized anxiety disorder (GAD) or Clinical Anxiety (CA), in which the situation triggering anxiety is not congruent with the manifestations of the latter (Lee et al., 2009b). This is evaluated using the Beck Anxiety Inventory (BAI; Beck et al., 2011).
A trait is a unit of personality, a dynamic behavioral tendency resulting from the integration of several specific habits of adjustment, expressing a characteristic mode of reaction of the individual in a given context (Allport, 1927). According to the DSM, personality traits are persistent patterns of ways of thinking, relating, and acting towards the environment and oneself that occur in a range of social settings. Various classifications of personality traits have been described (Cattell, 1943; 1945). According to Eysenck (1947), personality traits (PT) comprise four behavioral characteristics of individuals, related to ascendance (dominance and leadership), responsibility, emotional instability-anxiety, and sociability. These behavioral characteristics are grouped into two broad opposite traits: neuroticism (N), which correlates negatively with ascendance and self-esteem, and positively with emotional instability-anxiety, and extraversion (E), which correlates positively with ascendance and sociability (Eysenck, 1947; Eysenck et al., 1985). Because these behavioral tendencies have a high biological predisposition, it is difficult to tease apart the dimensions of anxiety and personality traits (Cattell & Scheier, 1958; Eysenck, 1963; Hettema et al., 2004).
Particularly in the case of young students in the areas of health sciences, the academic workload, as well as social, economic, and familial pressure during the protracted COVID-19 lockdown, constituted powerful stressors (Wathelet et al., 2020; Medina-Mora et al., 2022). Thus, the prevalence of stressful conditions, in conjunction with PTs, modulated by biological systems, result in states of anxiety in its different dimensions (Lee et al., 2009b; Caspi et al., 2010; Hansell et al., 2012). Indeed, it is known that daily exposure to various situations of emotional stress affects cognitive aspects of attention, interpretation and memory that facilitate the onset and maintenance of anxiety (Clarke et al., 2008), resulting in the poor academic performance of individuals, especially those of school age (Vilaplana-Pérez et al., 2021). However, it is unclear to what extent personality type determines the likelihood of presenting with anxiety. Establishing associations between PT and the various dimensions of anxiety in young students will therefore make it possible to enhance our knowledge of the interaction between personality and anxiety presented by youth and how this interaction could influence or impact emotional problems, as well as the cognitive and behavioral alterations prevailing in this sector of the population (Lee et al., 2009a).
Given the difficulty of teasing apart personality traits from anxiety dimensions, the hypothesis of this paper was that the neuroticism personality trait would present different degrees of correlation and prediction with anxiety dimensions depending on sex, age, and academic performance in young students from the state of Jalisco during the pandemic.
It was also hypothesized that the detection of personality traits predicting anxiety dimensions and dysfunctional behavioral patterns in young students would allow the use of early intervention strategies.
METHOD
Study design
This was a cross-sectional study with non-probabilistic sampling, conducted in the state of Jalisco, Mexico in May 2021.
Participants
The first step was to invite all the students enrolled in the psychology, nursing, and nutrition degree programs (young women and men ages 18-30) at two university centers: the University of Guadalajara, Ciénega de Ocotlán campus (CUCI UDG) and the University of Specialties Health Sciences campus (UNE). Students were informed that this was a research study, which complied with ethical guidelines, and had been previously authorized by the Ethics in Research Commission of the Institute of Neurosciences, based on NIH guidelines. All study participants voluntarily answered the survey.
Procedure
Information was provided through a link sent via email and social networks. Students were invited to participate on the understanding they could drop out of the survey if they so wished. In addition, they were informed that the data collected in this study would be held anonymously and be for the exclusive use of the laboratory.
Participants were told that this was an individual self-assessment survey, and that there were no right or wrong answers. They were asked not to spend a lot of time answering each question and to attempt to provide the answer that best indicated how they described themselves.
Google Forms was used for the virtual administration of the three anxiety scales, as well as the personality traits scale. Once participants had opened the link, they were able to access the information section, as well as the questionnaires and inventories required to ensure that they met the inclusion criteria, which began with a sociodemographic questionnaire with questions on their age, sex, and grades. Immediately afterwards, instructions for answering each inventory appeared on the screen. The instructions were as follows: “Read every sentence and fill in the numbered circle indicating how you feel usually or right now” according to the question. First, the 21-item Beck Clinical Anxiety Inventory (BAI) appeared. This was followed by the State-Trait Anxiety Inventory (STAI), comprising twenty items for TA and 20 for SA, and finally, a screen with the 24-item personality questionnaire. Once students had completed the survey, a thank you message appeared on the screen, indicating the end of the survey. The link closed and the results were automatically saved.
Scales and questionnaires
The Beck Anxiety Inventory (BAI) is a scale measuring the severity of clinical anxiety in adults and adolescents. The twenty-one items in the BAI contain the DSMV symptomatic criteria for the diagnosis of clinical anxiety, (including anxiety or panic attacks), for the last week including the day of the survey (Beck et al., 2011). In this paper, scores of 0-7 were described as “minimal CA.” Scores of 8–15 were termed “mild CA.” Scores of 16-25 were classified as “Moderate CA” and lastly, scores of 26-63 were described as “Severe CA” (Beck et al., 2011).
The State-Trait Anxiety Inventory (STAI) adapted to the Mexican population (Spielberger & Díaz-Guerrero, 2002) was used to measure the two dimensions of anxiety. The STAI Inventory has a section to assess trait anxiety (TA) consisting of twenty affirmative statements describing how the participant usually feels, whereas in the section to assess state anxiety (SA), the twenty expressions indicate how the participant feels at that moment (right now). Participants who obtained a score over 44 were considered to be in the TA or high SA group, while those who obtained a score below 30 were considered to be in the TA or low SA group (Spielberger & Díaz-Guerrero, 2002).
The present study was conducted in two phases.
In the first phase of the study, personality traits were assessed using the revised Eysenck personality questionnaire, abbreviated form (EPQR-A; Francis et al., 1992). The latter consists of twenty-four items divided into four dimensions of six items per subscale: extraversion (E), including aspects of positive emotionality, sociability, spontaneity, vitality and externalization; neuroticism (N), including traits such as negative emotionality, anxiety, sensitivity, worry, and self-consciousness; psychoticism (P), encompassing aspects of cruelty, impulsivity, low socialization, nonconformity, irresponsibility and schizoidism, and finally, dissimulation or lying (L), referring to the propensity to conceal or lie (Eysenck et al., 1985). A Likert-type scale response format was used (Muñiz et al., 2005), while the dispersion for each subscale varied from a minimum of four to a maximum of twenty-four points with a median of twelve. In this paper, direct scores were obtained from each subscale, without T transformation.
In the second phase of the study, only one personality trait, neuroticism (N), was evaluated using the revised Eysenck personality questionnaire, with twenty-four items corresponding to the complete EPQR-N neuroticism subscale, with dichotomous responses (Yes/No); and a maximum score of twenty-four (Eysenck et al., 1985).
To determine which personality trait contributed or explained the most in each of the dimensions of anxiety in the study participants, a sample of 185 students classified into different groups by age, sex and school grade were included in the first phase. CA, TA, SA, and Personality Trait scores were determined with the abbreviated scale (EPQR-A) for N, P, E and L using the scales and questionnaires mentioned earlier.
Due to their low contribution and to prevent oversaturation of the predictive model, to obtain a simplified model with the contribution of valid and replicable predictions, the elimination of PTs that contributed little to predicting anxiety dimensions was proposed. For each predictor introduced into the model, adjusted R2, there was a penalty since it depended on the degrees of freedom.
Data analysis
The reliability of the scales was established with Cronbach’s alpha (Cronbach, 1951). The raw total scores of Beck’s Anxiety Inventory, Spielberger’s State-Trait Anxiety Inventory (STAI) and the Eysenck Personality Profile Inventory were described and compared between groups (two age groups 18-24 and 25-30 years), two groups by sex (men and women) and three groups by grades (70-80, 81-90 and 91-100) as categorical independent variables. The difference between the theoretical and observed cumulative distribution of the variables described was calculated with the Kolmogorov-Smirnov (KS) test, to determine which statistic to use to compare the differences in means or medians and standard deviation (SD) or ranges. When there were two independent groups and normal distribution according to KS, the parametric T-test was used. If the distribution was not normal according to KS, non-parametric, Mann Whitney U test was used. For three groups, according to their distribution, one-way ANOVA was used, followed by Tukey’s test. Values of p < .05 were considered significant.
Using multiple linear regression analysis and statistics to determine whether there was collinearity with the Durbin-Watson test, the correlation (R) and the coefficient of determination (R2) were calculated as a predictor of anxiety dimensions with all PTs, in addition to sociodemographic variables. IBM SPSS Statistics 25 was used.
The sample size was calculated using the latest version of G*Power (v 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). With a power (1-β) of .80, and a significance level (α) of .05, for a bivariate Pearson linear correlation analysis (with an a priori calculation from the worst-case scenario of a low correlation of 0.2), a sample size of 193 subjects would be required. However, based on previous studies in which a correlation of neuroticism with trait anxiety of .848 and of .70 with state anxiety was obtained (Eid et al., 2022), the necessary sample size was eight to thirteen subjects.
Ethical considerations
None of the procedures in this non-invasive research posed a risk to the physical, emotional, or moral integrity of the participants. The research therefore qualifies as minimal risk in accordance with Article 17 of the Regulations of the General Health Law on Health Research. In addition, the guidelines specified in the 1975 Declaration of Helsinki and its amendments were followed, as well as current international codes and standards for good practices in research with humans, and the Official Mexican Standard NOM-012SSA3-2012, which establishes the criteria for undertaking research projects for health in human beings.
This project was approved by the Ethics Committee of the Institute of Neurosciences of the University of Guadalajara, with registration number ET022021-314.
RESULTS
Phase 1
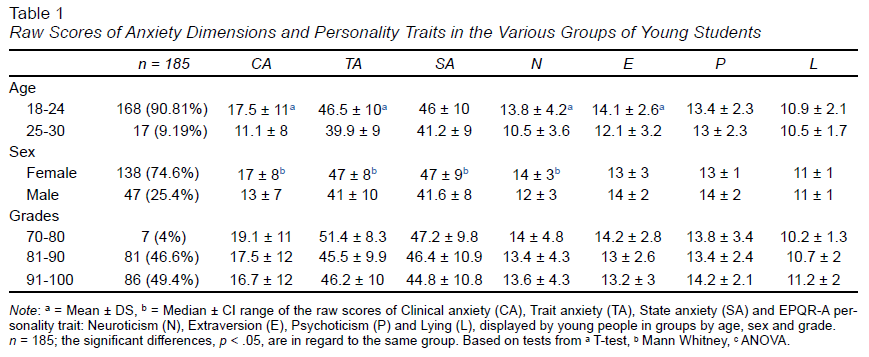
Subjects who did not fall within the age range of 18 to 30 or failed to complete the survey were eliminated. Of the 185 participants who completed the entire survey at various university centers in the state of Jalisco, Mexico, with an average age of 21 (± 2.6) years, 74% were women; It was found that those under 24 and women had a higher total score for CA, as well as TA and SA. Students with lower grades had higher total CA and SA scores. Participants under 24 and women also displayed higher PTs for neuroticism (Table 1).
The reliability found in the Phase 1 sample of 185 participants or Cronbach’s alpha coefficient was .923. for the BAI CA scale, .888 for the STAI TA, .913 for the STAI SA and .823 for the EPQR-A personality traits.
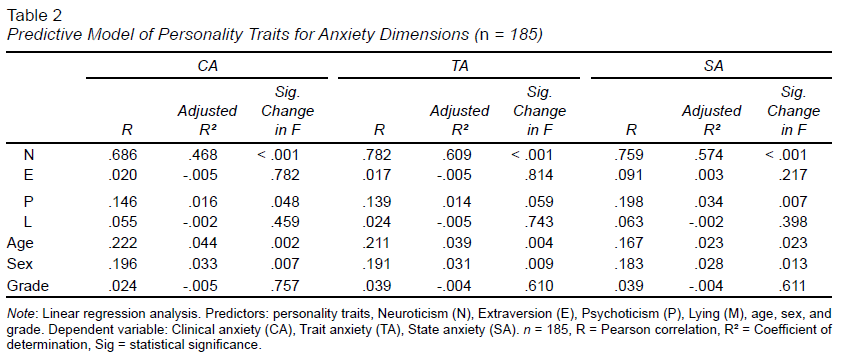
Subsequently, to determine and predict how much each of the personality traits contributed to the anxiety dimensions, a multiple linear regression analysis was conducted, with statistics to determine whether there was collinearity. The correlation and determination coefficient were determined, using the four personality traits, age, sex, and grades, as predictor variables for each of the dimensions of CA, TA, and SA as dependent variables. Values of p < .05 were considered significant. All of the above was analyzed using SPSS Statistics 25.
The predictor values for CA, TA, and SA are described in Table 2. As can be seen, the neuroticism personality trait achieved the highest statistically significant predictor value, indicating that this personality trait contributes most to the presence of CA, TA, and SA. Psychoticism, age, and sex only contributed minimally while the other traits provided little or no predictive value.
Phase 2
According to the results of Phase 1, the neuroticism personality trait is the one most strongly associated with the various dimensions of anxiety. Thus, based on the results of Phase 1, a second phase of sampling and analysis was conducted, with a sample of 521 students also classified into different groups by age, sex, and grades. In this sample, the CA, TA, SA, and Personality Trait scores were also determined, but only with the complete neuroticism subscale (EPQR-N; Eysenck et al., 1985) to be able to associate and predict how much neuroticism contributes to each of the dimensions of anxiety. To this end, a Pearson linear regression analysis and coefficient of determination (adjusted R2) were applied, to show how much neuroticism predicts the dimensions of anxiety.
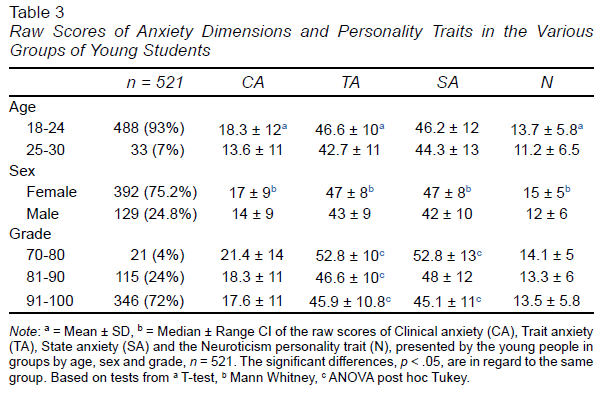
As in phase 1, a demographic description of the participants was made, shown in Table 3. Subjects who did not fall within the age range of 18 to 30 or failed to complete the survey were eliminated. In the end, a total of 521 students from various university centers in the state of Jalisco, Mexico participated. Enrolled in the areas of Health Sciences, students had an average age of 20.5 (± 2.3) years, and 75.2% were women and 24.8% men. It was found that those under 24 and women had a higher total score for CA, as well as for TA, while only women had SA. Students with lower grades had higher total CA and SA scores. Participants under 24 and women also displayed higher PTs for neuroticism (Table 3).
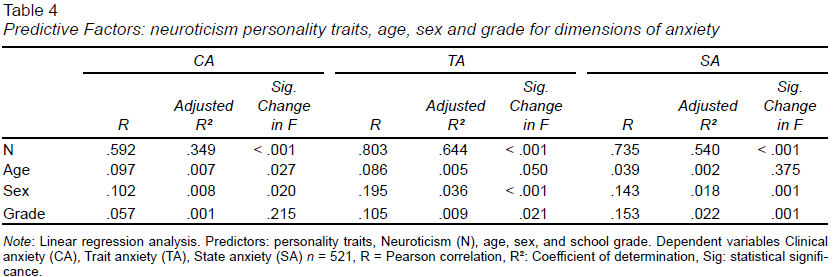
As with the data from Phase 1, a regression analysis was conducted to determine the correlation and determination coefficient, using only the data from the complete neuroticism scale (EPQR-N), age, sex, and grades, as predictor variables for each of the dimensions of CA, TA, and SA as dependent variables. As can be seen in Table 4, demographic variables (age, sex, and school grade) contributed little to predicting the dimensions of anxiety.
In addition, a regression analysis was conducted to determine the final predictive model using only data from the complete neuroticism scale (EPQR-N) as a predictor variable and the anxiety dimensions as dependent variables: CA, TA, and SA.
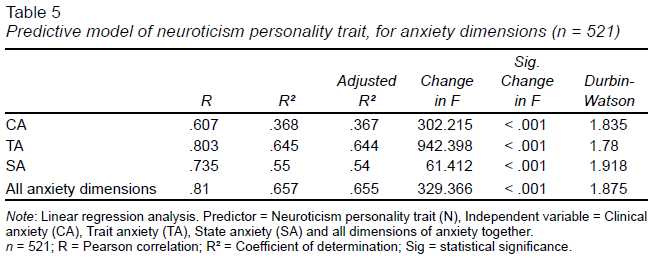
It was found that the neuroticism personality trait contributed to the various dimensions of anxiety, in varying proportions: .367 for CA, .644 for TA and .540 for SA. Likewise, it was found that neuroticism predicts all dimensions of anxiety with a coefficient of determination (adjusted R2) of .655 (Table 5).
DISCUSSION AND CONCLUSION
An individual’s personality trait is derived from the interaction of a series of genetic and environmental factors, characterizing the differences found in each individual (Vukasović & Bratko, 2015; Gross & Hen, 2004). This paper found that the biological personality trait characterized by negative emotionality, neuroticism, contributed most to the presence of anxiety in its various dimensions with a proportion of over 60% in TA, surpassing other factors such as sex, age, grades, or other PT showing predictive independence.
From the 1940s onwards, Eysenck made significant contributions to the description of human PTs (Eysenck, 1944; 1947; 1963; Eysenck et al., 1985), a classification that has continued to be used until the preset (Eysenck, 2016). His contribution laid the foundations for determining that individual differences in personality traits are associated with cognitive processes and neural networks (Eysenck, 1997; Saviola et al., 2020). These individual differences in personality traits determine the way situations are perceived as threatening and the anxiety response. Knowing the personality trait of everyone would therefore make it possible to predict their anxiety reaction to a threat.
The results of this work show that the neuroticism PT is most strongly associated with the presence of the three dimensions of anxiety in the students in health areas in our sample. These results coincide with what has been reported by Bienvenu & Stein (2003) and other authors (Bienvenu & Stein, 2003; Brandes & Bienvenu, 2006; Kotov et al., 2007), who found that certain PTs are associated with the presence of anxiety, neuroticism being the one most associated with anxiety disorder; However, they did not distinguish between the three dimensions of anxiety, which is the original contribution of the present study.
Other research has reported that the biological personality trait neuroticism is genetically associated with anxiety (Hettema et al., 2004; Barlow et al., 2014; Zugliani et al., 2017). Our results show that the greatest correlation and predictive value of neuroticism is with the presence of TA (Clarke et al., 2008; Uliaszek et al., 2009; Zugliani et al., 2017). The high correlation obtained in our sample was probably due to the fact that neuroticism and TA share common features, as has been suggested by other authors (Uliaszek et al., 2009).
Likewise, the results of other reports concur with ours. These reports observe an even smaller contribution than the one we found in this paper of neuroticism to the prediction of the manifestations of clinical anxiety or panic, which can alter physical homeostasis. If left uncontrolled, its intense, recurrent manifestations can result in severe generalized anxiety disorder (Jorm et al., 2000; Brown & Naragon-Gainey, 2013; Zugliani et al., 2017; Pérez-Mengual et al., 2021).
In general terms, women were found to have a greater prevalence and severity of manifestations of dimensions of anxiety, coinciding with other studies in which sex differences in personality and anxiety traits are reported in all its dimensions (Hettema et al., 2005; Gottschalk & Domschke, 2017).
Our data differ from those found by Eid et al. (2022) who reported differences between TA and SA with values similar to those obtained in our group of young people. Neuroticism was found to contribute to a lesser extent to the momentary reaction of SA in participants’ self-reports.
One of the most striking results of the present study is that overall, a higher prevalence of anxiety was found than that reported by other authors (Wathelet et al., 2020; Vahratian et al., 2021; Santomauro et al., 2021; Medina-Mora et al., 2022). This difference is probably due to the restrictive conditions of the pandemic experienced between 2020 and 2021. The lack of information on the conditions and aspects of how each participant experienced lockdown, and only having answers obtained virtually, making it impossible to control the way the surveys were administered (ideally individually and in a setting with no distractions), meant that the data compilation was out of our hands.
For over twenty years, mental health has been a priority in the surveillance and treatment system for the WHO, due to the fact that a considerable increase in emotive-emotional diseases has been reported (Twenge, 2000). And in Mexico, the National Survey of Psychiatric Epidemiology (ENEP) has reported an over two-digit increase in the prevalence of anxiety disorders (Medina-Mora et al., 2003; Benjet et al., 2016; Medina-Mora et al., 2022), underlining the importance of establishing more controlled monitoring mechanisms nationwide.
Although the results obtained in the present study only constitute a sample of the high correlation between the neuroticism PT and the presence of anxiety in the youth population of the state of Jalisco, these data provide evidence of the severity of this health problem that probably occurs at the national level, particularly among young students in the area of health sciences. There is therefore an urgent need for the health system and the family nucleus to design more strategies to support and prevent anxiety especially in subjects with high biological vulnerability due to their neuroticism personality trait, which, together with external factors such as the pandemic and its consequences, increased the prevalence of the dimensions of anxiety among young people in the state of Jalisco.